The thalamus, which is involved in the processing of sensory inputs and almost all interactions among cortical, subcortical, and brainstem nuclei, is of major interest in schizophrenia. Investigators have speculated that a thalamic abnormality could be associated with the deficiencies in filtering stimuli, focusing attention, or sensory gating reported in schizophrenia
(1–
5). Andreasen et al.
(2) hypothesized that the signs and symptoms of schizophrenia could be explained by abnormalities in midline structures that modulate attention and information processing, particularly the thalamus and its related circuitry.
Postmortem neuropathology in schizophrenia has shown a loss of volume and cell number in the thalamus
(6–
9), especially in the mediodorsal nucleus
(8,
9). Synaptic degeneration in the thalamus
(10), reduced parvalbumin-immunoreactive thalamocortical projection neurons
(11), and chromatolytic change in the medial thalamus
(12) have also been reported. The mediodorsal nucleus is of particular interest because it serves as a major cortical relay from the limbic system and has connections to the prefrontal cortex
(13).
Magnetic resonance imaging (MRI) studies have generally shown a reduction in thalamic size in schizophrenia (see reference
14 for review). The earliest study
(15) found a trend for the thalamus to be smaller in male patients than in comparison subjects (p=0.05), a difference that reached significance for both sexes in a later study with more subjects
(16). While a study by Andreasen et al.
(2) that used an image-averaging approach suggested a loss of volume in the lateral thalamus, change in the adjacent internal capsule, or both (see discussion in references
1 and
17), limits of resolution did not permit the determination of which specific nuclei were affected. A combined MRI/positron emission tomography (PET) study revealed no significant decrease in whole thalamic area, but shape analysis suggested decreased left anterior and right posterior size
(1). A family study found the left thalamus to be smaller in relatives of schizophrenic patients than in normal subjects
(18). Reduced thalamic area was also reported in childhood-onset schizophrenia
(19,
20), with a continued decrease over 2-year follow-up. In a study of patients with late-life schizophrenia (average age=59 years), divided into subgroups with early (before age 45) or late (after age 45) onset of illness, reduced thalamic volume was found in patients with early-onset schizophrenia, whereas increased thalamic volume characterized patients with late-onset illness
(21). Portas et al.
(22) outlined the thalamus on coronal sections and did not find whole volume decreases.
Previous PET studies that examined the thalamus in schizophrenia have produced mixed findings. In comparisons of schizophrenic and normal subjects, studies variously found thalamic metabolic rates in schizophrenia to be higher (in adults
[23] and adolescents
[24]), lower
(1,
25,
26), lower in patients with the deficit syndrome only
(27), or unchanged
(28–
32). There are two important possible explanations for the disagreement among studies. First, PET findings could be affected by the use of varied uptake conditions. Different tasks may involve activation to varying degrees of different thalamic nuclei, as well as the corresponding afferent or efferent brain regions connected to a specific nuclear group. In a study that used a task requiring sustained attention—the visual continuous performance test—we found that the anterior nucleus, which has a major output to the cingulate gyrus
(33), had lower activity in schizophrenic than in normal control subjects
(1). A task with a cognitive focus different from that of the continuous performance test might reveal abnormalities in a region of the thalamus other than the anterior nucleus. For example, previous work linking a deficit in the formation of long-term memory to mediodorsal thalamic lesions
(34,
35) suggests that schizophrenic patients might show mediodorsal dysfunction during a verbal memory task.
Second, methodological problems could have confounded the strength of differences between normal and schizophrenic subjects
(1). With two exceptions
(1,
24), all studies assessed thalamic function on the basis of coordinates placed visually or stereotaxically in the center of the thalamus. For example, region of interest placement in the center of the thalamus by stereotaxis may blur or lump together thalamic nuclei with different functions. The possibility that certain thalamic nuclei, such as the anterior and mediodorsal nuclei, which have reciprocal connections with frontal lobe structures, may be key in schizophrenia
(36) underlines the need for precise localization. Individual differences among patients and comparison subjects in size, shape, and position of the thalamus could obscure findings in studies that rely on stereotaxis to define regions of interest. For more precise comparison of regions of the thalamus, an MRI-derived three-dimensional anatomical template would facilitate reliable identification of thalamic regions.
The major goals of this study were threefold.
1. Enhanced spatial resolution. We wanted to extend our previous work with 7.5-mm full width at half maximum PET and a two-dimensional 5-mm-thick MRI template in a new and larger group of patients by using both higher-resolution PET (4.5 mm full width at half maximum) and three-dimensional coregistered 1.2-mm MRI. This methodology provides more precise localization of the thalamus, which is necessary to elucidate the subregions that are hypothesized to be dysfunctional in schizophrenia.
2. Memory function. Because our past work primarily used a visual vigilance task, the continuous performance test, we decided to tap additional functions of theoretical relevance by using a serial verbal learning task that requires both short-term (i.e., working memory) and encoding for long-term memory and is related to the literature on the various thalamic nuclear groups and their respective connections.
3. Schizophrenia spectrum. We wondered whether thalamic abnormalities in schizophrenia would also characterize schizotypal personality disorder. Because schizotypal personality disorder is genetically related to schizophrenia
(37), inclusion of this patient group could help clarify our understanding of deficits that are central to the pathophysiology of schizophrenia. Possible biological markers in schizotypal personality disorder are less likely to be affected by contaminating influences of histories of antipsychotic drug treatment and hospitalizations. Since no previous study has examined thalamic size, shape, or function in schizotypal personality disorder, it appeared valuable to address this gap in the literature.
METHOD
Participants
Twenty-seven schizophrenic patients (20 men and seven women; mean age=38.3 years, SD=14.3) were evaluated with the Comprehensive Assessment of Symptoms and History
(38) and were diagnosed as having schizophrenia (N=24) or schizoaffective disorder (N=3), according to DSM-IV. Patients were neuroleptic naive (N=7) or neuroleptic free for a median of 3 weeks (N=20; 15 men and five women; none had taken long-acting neuroleptics; shortest washout=12 days; next shortest=14 days; longest=3 years). Total scores on the 18-item Brief Psychiatric Rating Scale (BPRS)
(39) were obtained for 25 of the patients on the day of their PET scan (mean=54.4, SD=12.1; range=30–85; minimum possible rating=18).
Thirteen patients with schizotypal personality disorder (12 men and one woman; mean age=43.3 years, SD=13.6) were interviewed with the Schedule for Affective Disorders and Schizophrenia
(40)and the Structured Interview for DSM-III-R Personality Disorders
(41). All met DSM-IV criteria for schizotypal personality disorder. Mean total BPRS score (N=12) was 37.5 (SD=6.2; range=28–46).
Thirty-two normal control subjects (25 men and seven women; mean age=41.8, SD=12.1) received a Comprehensive Assessment of Symptoms and History interview to exclude psychiatric illness in themselves or first-degree relatives. Both patients and volunteers were screened as described elsewhere
(42). After a complete description of the study to all subjects, written informed consent was obtained.
PET [18F]Fluorodeoxyglucose (FDG) Uptake Task and Procedure
Intravenous lines were inserted in the left arm for blood sampling and the right arm for FDG injection. After placement of intravenous lines, participants were moved to a comfortable chair in a sound-attenuated room. Before the procedure, participants were read standard instructions about the serial verbal learning task, which was developed for the 32-minute FDG-uptake period and is analogous to the California Verbal Learning Test
(43). The serial verbal learning task comprised five 16-word lists, each containing four words from four semantic categories (e.g., fruits, clothing, colors, spices). A more detailed description is provided elsewhere
(42). Scores were recorded for total number of correctly recalled words, recall by semantic clustering versus serial ordering, intrusions (words not in list), and perseverations (repetition of word on the same trial).
PET and MRI
PET scans (20 slices, 6.5-mm intervals) were obtained with a head-dedicated GE scanner (model PC2048B) with measured resolution of 4.5 mm in plane (4.2–4.5 mm across 15 planes). T1-weighted axial MRI scans were acquired with the GE Signa 5x system (TR=24 msec, TE=5 msec, flip angle=40°, slice thickness=1.2 mm, pixel matrix=256×256, field of view=23 cm, total slices=128).
PET and MRI Coregistration
The PET and MRI scans were obtained in the axial plane (canthomeatal line) through use of the same individually molded thermoplastic head holder. PET scans were coregistered to MRI by using brain slice edges
(44). PET edges were automatically generated following image smoothing with a radial threshold-seeking algorithm on all 20 PET slices. MRI edges were hand drawn on the brain edge by identifying 50–100 points and passing a best-fit spline curve through the points. MRI within-edge area was assessed in 10 subjects from the current group, traced by two independent tracers, which yielded an intraclass correlation coefficient (ICC) of 0.98
(45). Accuracy was tested by scanning a subject with capillary tubes that were fastened to the face and were filled with a mixture of copper sulfate (0.5 M) and FDG; the resulting distance between the two marker centers (FDG and copper sulfate both outside and independent of the traced edge) was 1.79 mm, compared with 1.83 mm reported by others
(44). Imaging and coregistration procedures are described in detail elsewhere
(42).
Tracing of the Thalamus on MRI
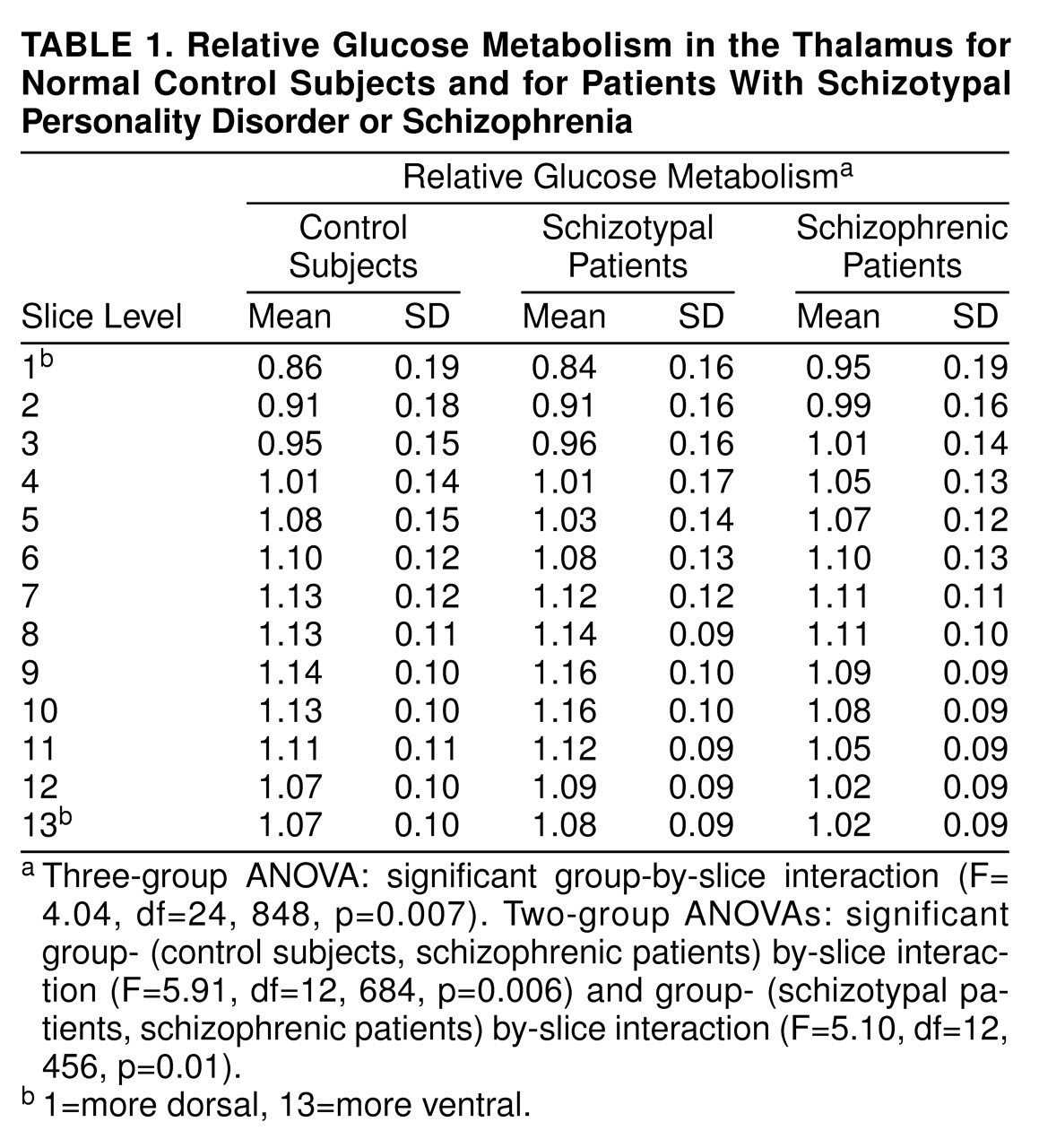
Thalami were traced on contiguous 1.2-mm axial MRI scans with tracing guidelines as shown (
Figure 1). To determine the reliability of tracing methods, two independent tracers examined right thalamus tracings from axial slice levels ranging from top to bottom of the thalamus for a subset of the current group (24 subjects). Intertracer reliability (ICC) for two tracers was 0.91 for area and 0.99 for relative metabolic rate. Intertracer overlap percentage was calculated as the number of pixels common to both tracers’ outlines multiplied by 100 and divided by the average number of pixels in each tracer’s outlines (94.5% for the thalamus).
For comparability with previous work
(1), the shape of the thalamus was examined by selecting, for each participant, one MRI slice that passed through the center of the thalamus in the z direction, matching a standard atlas at 41% of head height
(46).
Statistical Analysis
Two complementary approaches were used to analyze relative glucose metabolic rate (rGMR): analysis of variance (ANOVA) on thalamic slice levels and groups and significance probability mapping for an exploration of thalamic subregions. The ANOVA for rGMR used a three-group (control, schizophrenia, schizotypal personality disorder)×13 (slice: 1–13)×2 (hemisphere: right, left) mixed-factorial design. Average rGMR was calculated for left and right thalami as the mean activity value for all pixels in the region of interest divided by whole brain activity. A 3×2 mixed-factorial design was used for the thalamus-volume analysis. The first variable comprised three groups; the second, two hemispheres. Separate ANOVAs were done for absolute thalamic volume (in cubic millimeters) and relative thalamic volume (thalamic volume in cubic millimeters divided by brain volume in cubic millimeters). Thus, our statistical approach allowed 1) specific a priori hypothesis testing of mean rGMR within the MRI-based outline of the thalamus with a single F ratio (group by slice by hemisphere) to control type I error, and 2) pixel-by-pixel t test significance probability mapping
(47,
48) using the entire three-dimensional reconstruction of the thalamus. The significance probability mapping approach included a conservative resampling method
(49) to determine significance levels
(42,
50) with actual PET thalamus data from a pool of 30 additional normal control subjects (age- and sex-matched) studied under identical conditions. An empirical table of cluster volumes was created by generating 5,000 random samples from the total pool of 62 volunteers and obtaining the single largest cluster for each random draw. Volumes for the 0.05, 0.025, and 0.01 significance levels were obtained, permitting a test of whether any given pixel cluster volume might occur by chance if groups differed no more than random sets of volunteers.
All statistical analyses involving repeated measures with more than two levels used Greenhouse-Geisser epsilon corrections to adjust probabilities for repeated measures F values. We report here the uncorrected degrees of freedom for these analyses and for t tests that required correction because of heterogeneity of variance.
RESULTS
Thalamic rGMR
The three-way mixed-design ANOVA for rGMR in the thalamus (group [normal control subjects, schizophrenic patients, and patients with schizotypal personality disorder] by slice by hemisphere) confirmed a group-by-slice interaction (
Table 1). A significant main effect of slice indicated a dorsal-to-ventral gradient for thalamic rGMR across groups. The main effects of group and hemisphere and the other interactions were not significant. To determine how the two patient groups contributed to the significant group-by-slice interaction, two-group ANOVAs were conducted. A significant group-(control versus schizophrenia) by-slice interaction emerged in which schizophrenic patients showed lower rGMR in middle and ventral thalamus slice levels (slices 7–13) and higher rGMR in the most dorsal slices (slices 1–4) than volunteers (
Table 1). A significant group-(schizotypal personality disorder versus schizophrenia) by-slice interaction indicated a strikingly similar pattern of differences between the two patient groups. Last, no significant group effect or interaction with group was found in the three-way ANOVA comparing the normal control and schizotypal personality disorder groups.
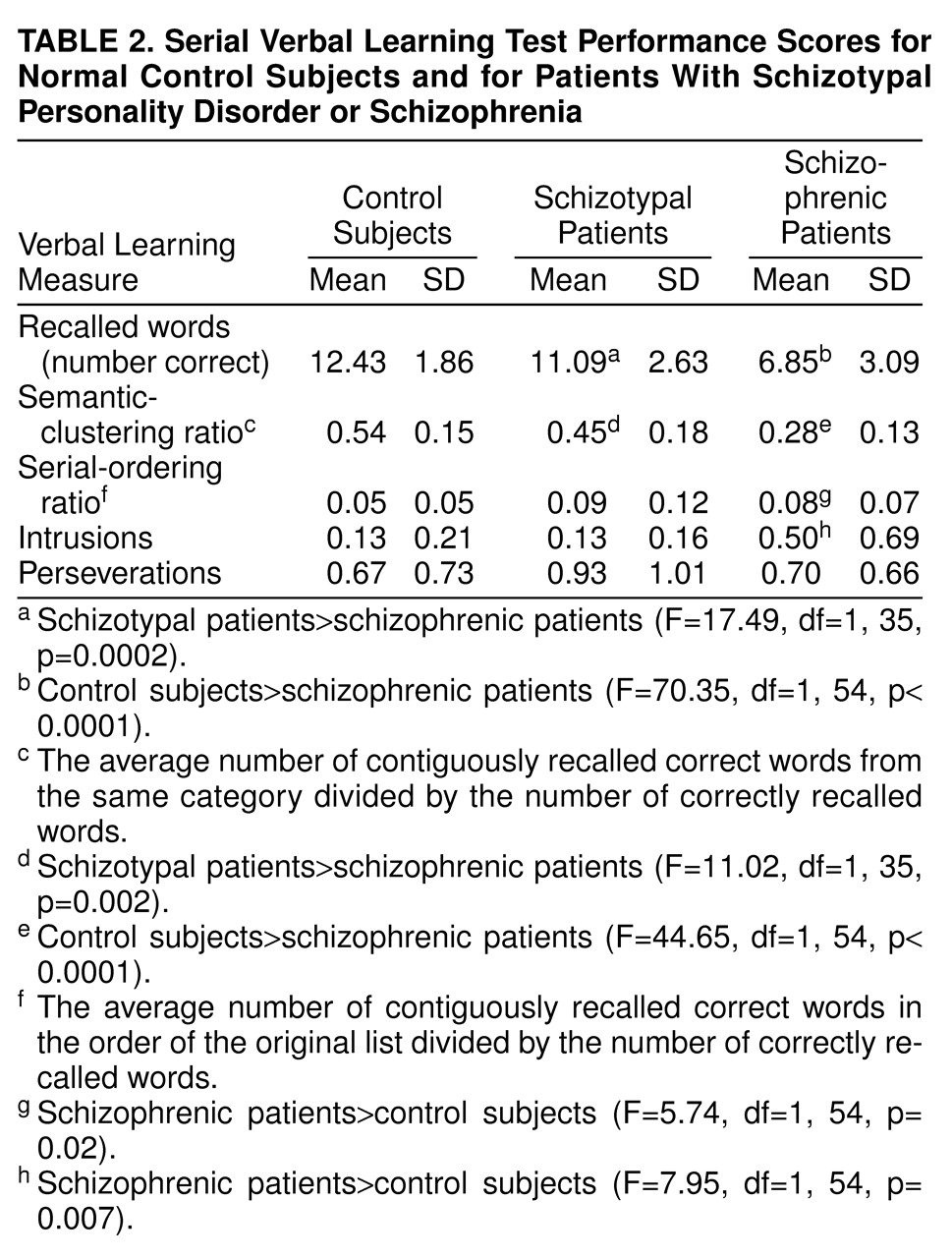
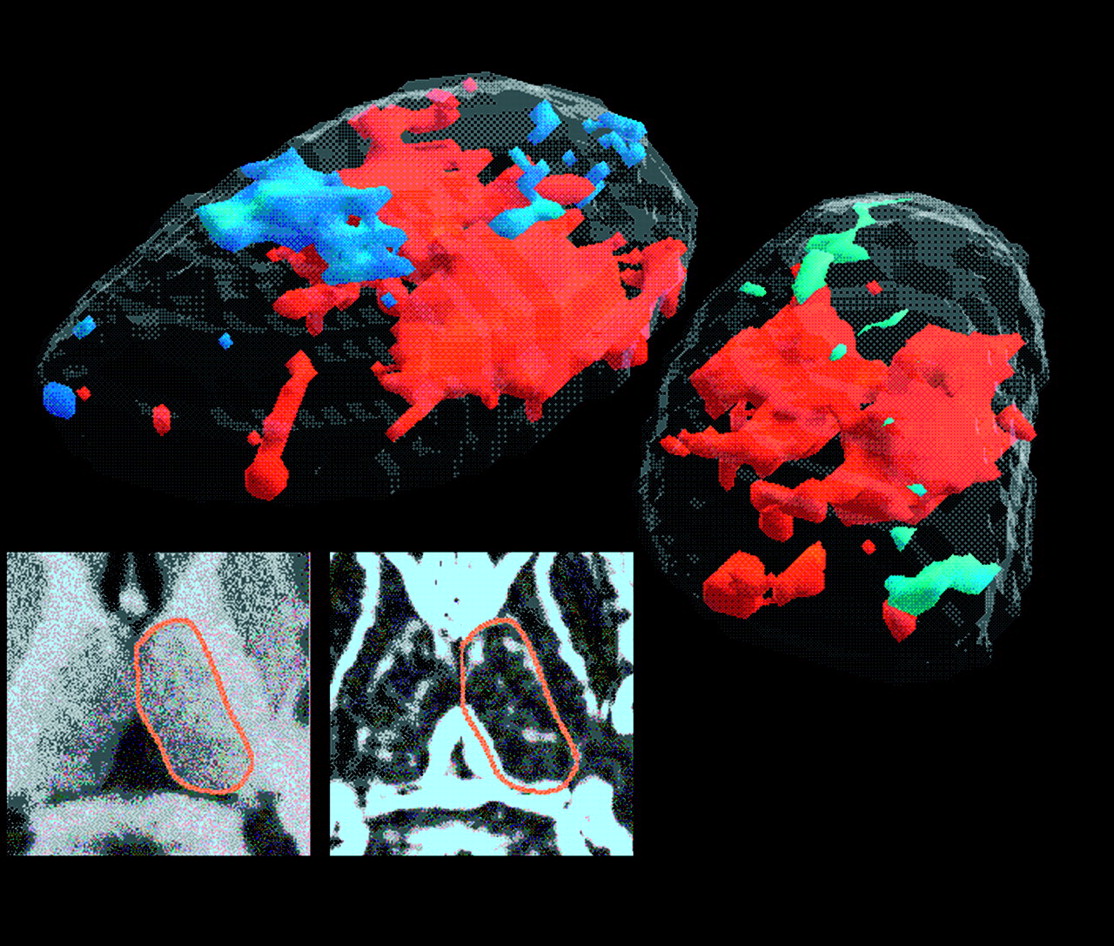
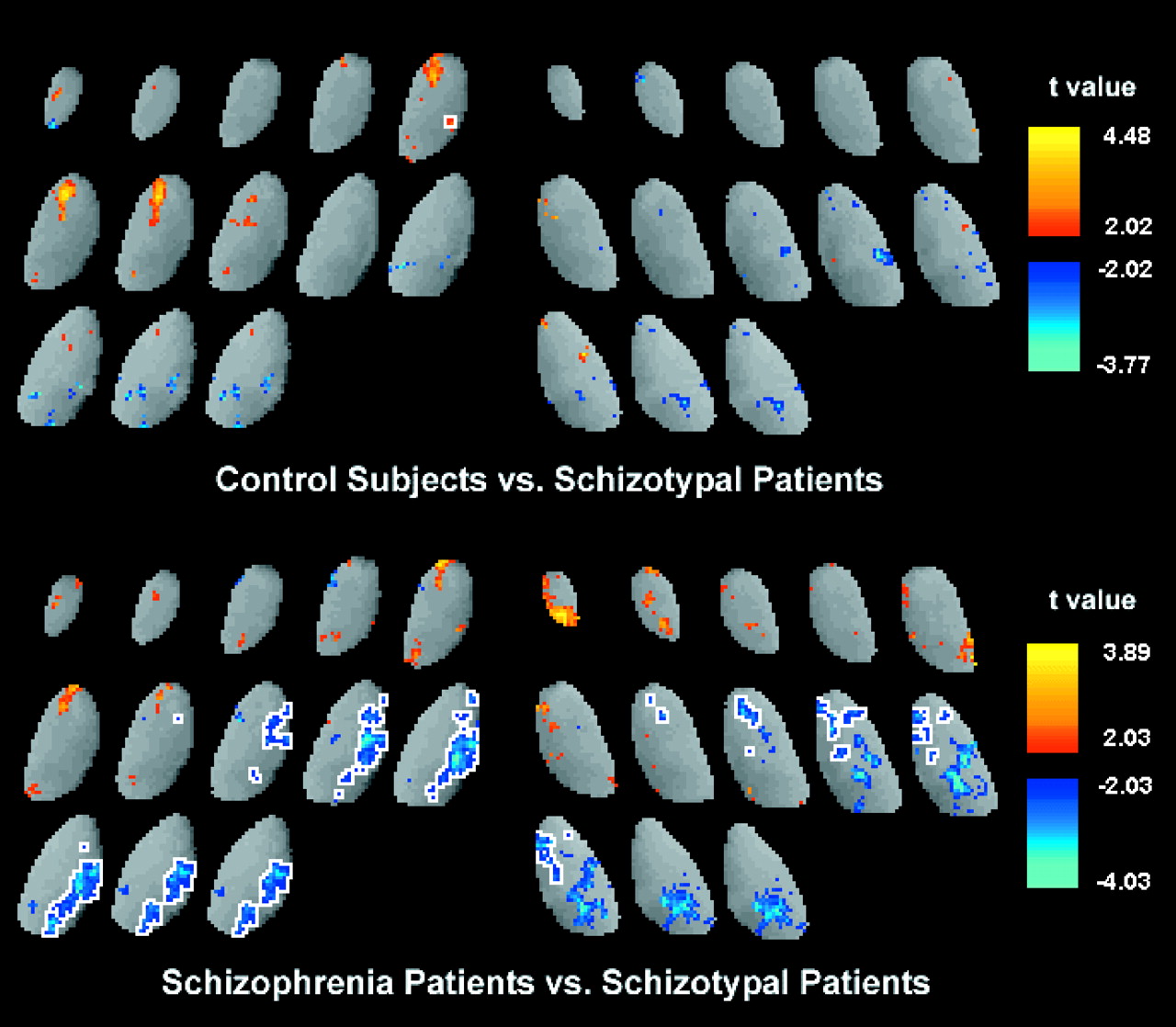
The significance probability mapping analysis comparing thalamic rGMR in control subjects and schizophrenic patients indicated that patients had significantly decreased metabolic rate, located primarily bilaterally in the region of the mediodorsal nucleus (
Figure 2). The significance probability mapping analysis comparing thalamic rGMR in the two patient groups (
Figure 3) revealed significantly lower rGMR, primarily in the mediodorsal region of the left and right thalami, in schizophrenic patients than in patients with schizotypal personality disorder. Last, the three-dimensional significance probability mapping analysis comparing control subjects and patients with schizotypal personality disorder revealed no significant difference in thalamic rGMR.
Size and Shape of the Thalamus
Analysis of total brain volume showed no significant difference among the three groups (control: mean=1318 cm3, SD=109; schizophrenia: mean=1272, SD=119; schizotypal personality disorder: mean=1390, SD=201; all t values<1.98, p>0.05). Absolute thalamic volume (average of left and right) did not differ significantly among the groups (control: mean=6221 mm3, SD=793; schizophrenia: mean=5904, SD=871; schizotypal personality disorder: mean=6085, SD=1040; F=1.06, df=2, 69, p=0.35). The group-by-hemisphere interaction also failed to reach significance (F=0.39, df=2, 69, p=0.68). Similarly, the three groups did not differ in relative thalamic volume [control: mean=0.473% (mm3 divided by brain volume in mm3], SD=0.06; schizophrenia: mean=0.466%, SD=0.07; schizotypal personality disorder: mean=0.442%, SD=0.07; F=1.23, df=2, 69, p=0.30); the interaction with hemisphere also was not significant (F=0.50, df=2, 69, p=0.61).
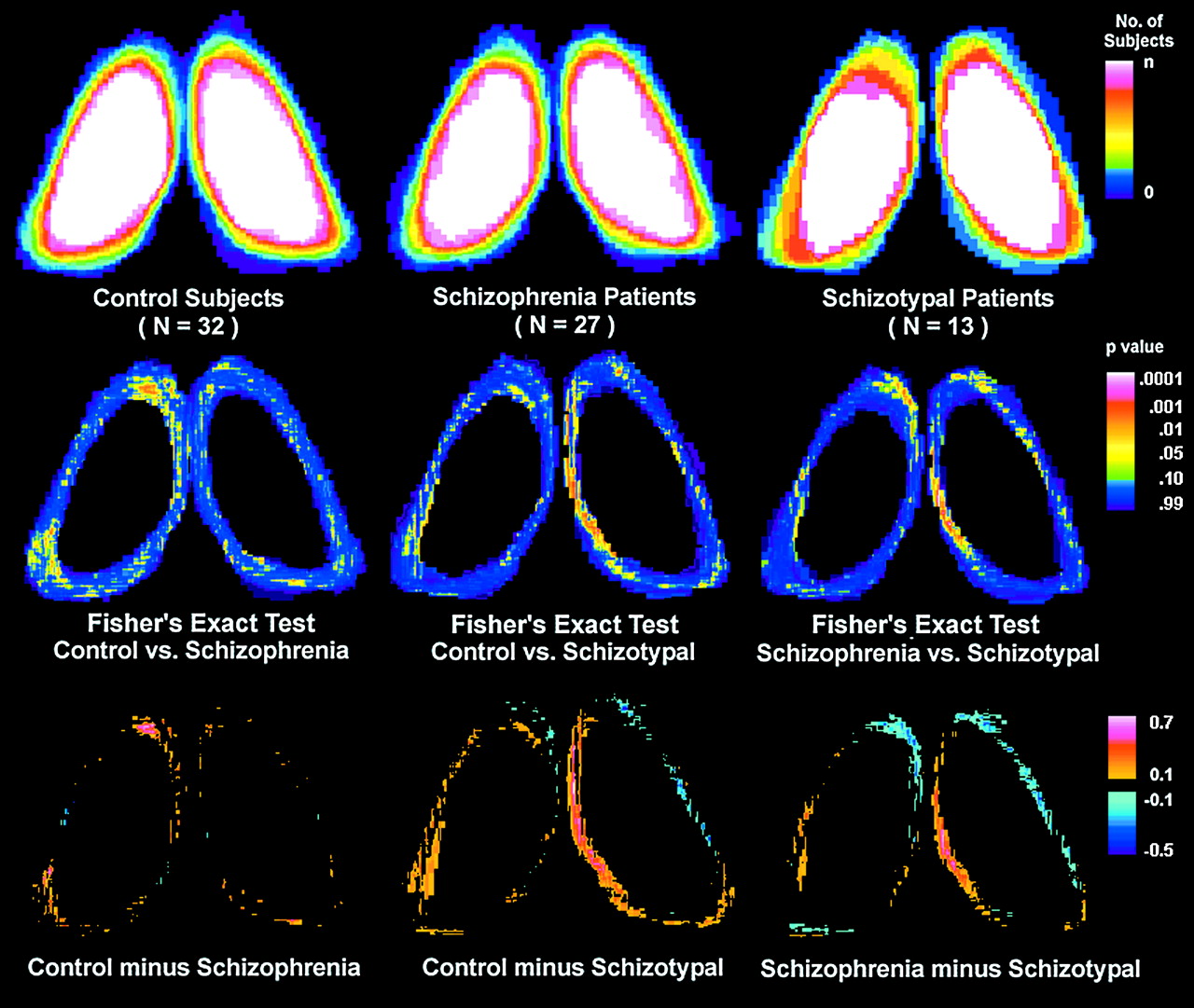
Figure 4 shows the statistical contour maps of thalamic shape for each group. Compared with control subjects, schizophrenic patients had significantly fewer pixels at the anterior tip of the left thalamus. Compared with both normal control subjects and schizophrenic patients, patients with schizotypal personality disorder had significantly fewer pixels in the region of the right mediodorsal nucleus (for all Fisher’s exact tests, p<0.05).
BPRS and Task Performance
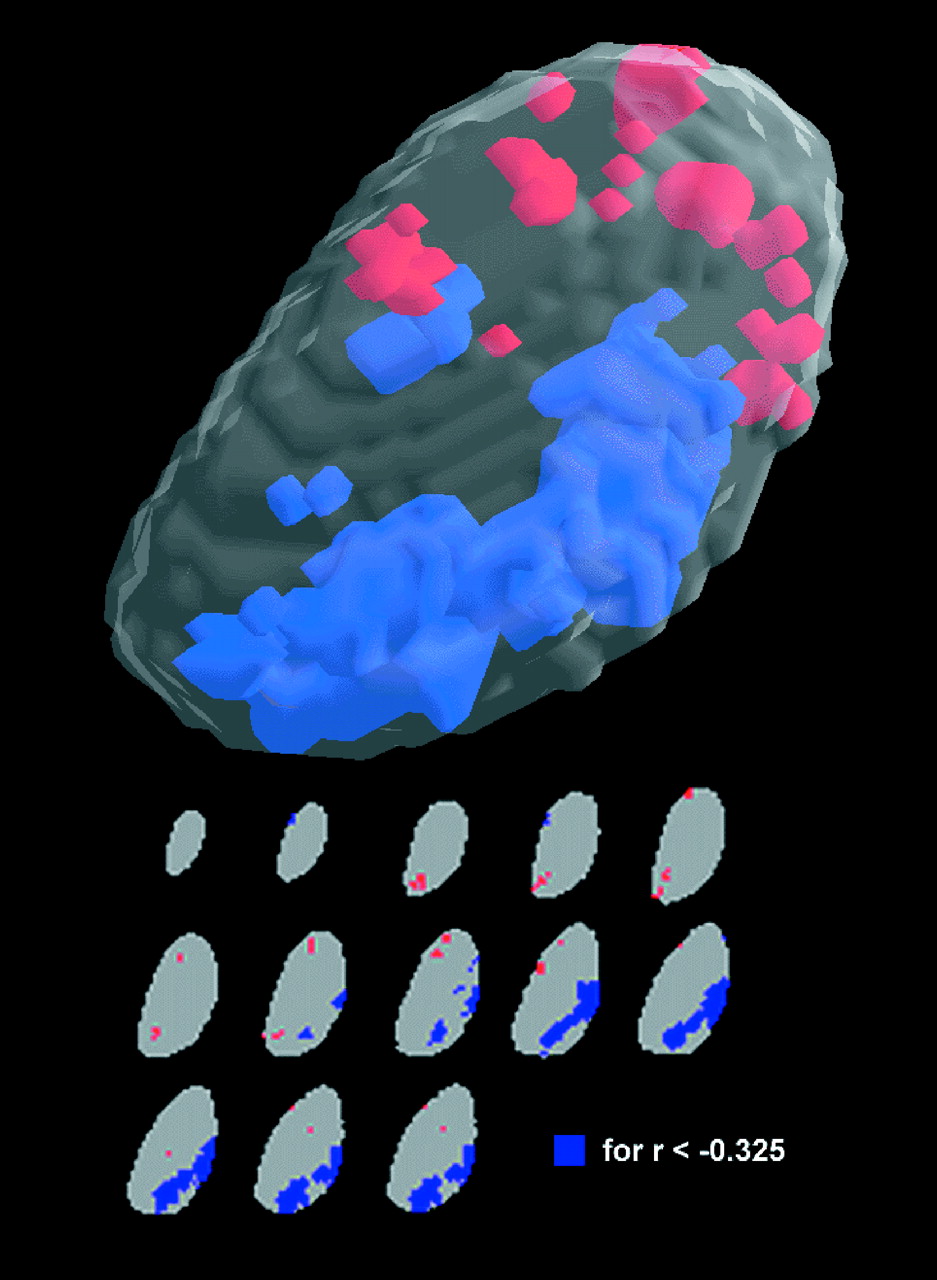
Among the combined groups with schizophrenia and schizotypal personality disorder, those with higher total BPRS scores on the day of the PET scan had lower metabolic rates in the region of the mediodorsal and pulvinar nuclei of the thalamus (
Figure 5).
Except for three schizophrenic patients who could not complete the task, all subjects were cooperative and performed at above-chance levels (analyses excluding patients who failed to finish the task did not change the imaging findings). Not surprisingly, both control subjects and patients with schizotypal personality disorder had better scores on most performance measures than schizophrenic patients. The control and schizotypal personality disorder groups recalled significantly more correct words and had significantly higher semantic-clustering-strategy scores than the schizophrenic group (
Table 2). In contrast, the schizophrenic patients had significantly higher serial-order scores than control subjects. Compared with the control subjects, patients with schizotypal personality disorder did not differ significantly on intrusion scores, whereas schizophrenic patients had significantly more intrusions. Last, the three groups did not differ on perseveration scores.
DISCUSSION
Our finding of diminished thalamic metabolism in schizophrenic patients compared with control subjects is consistent with previous findings (1, 25, 26, 51). However, this is the first study to show significantly decreased rGMR primarily located bilaterally in the region of the mediodorsal nucleus in schizophrenic patients. This finding is consistent with detailed neuropathological studies that have reported decreased neuronal density and volume reduction in the mediodorsal nucleus (8, 9). The mean volume of the medial dorsal nucleus, approximately 500 mm3 in postmortem brain (9), may be compared with the PET scanner resolution assessed with our measured full width at half maximum (slice center) of 122 mm 3 or four full width at half maximum volume. This places the medial dorsal nucleus in the range of moderate recovery coefficients. Patients with schizotypal personality disorder did not differ significantly from control subjects in thalamic rGMR and showed less severe symptoms than schizophrenic patients, suggesting that thalamic abnormalities may be related to symptom severity in the schizophrenia spectrum.
The lack of differences between schizophrenic and normal subjects in total thalamic volume is consistent with a recent volumetric MRI study (52), as well as with other work that examined thalamic area (see reference 14 for review). Our negative finding does not seem only to be the result of inadequate group size (N=59); we had 0.80 power to detect a 10% difference in volume. The observed control-versus-schizophrenia effect size was 0.38, which was only 4.7% of thalamic volume; with our group size we had 0.33 power to detect such a small volume effect. An earlier shape-analysis finding that the left anterior region of the thalamus is significantly smaller in schizophrenic than in normal subjects
(1) was replicated in the present study. Shape analysis also revealed significantly fewer pixels in the region of the right mediodorsal nucleus in patients with schizotypal personality disorder. Shrinkage of the brain in other areas may occur in patients with schizotypal personality disorder, as suggested by the ventricle abnormalities found in this same group of patients with schizotypal personality disorder
(53).
Abnormalities in the anterior and mediodorsal nuclei are of interest because of their connections with various other structures. The primary connections of the anterior nucleus are with limbic structures including the hippocampus and cingulate gyrus. The anterior nucleus receives substantial input from the hippocampus by means of the fornix, and the hippocampus has been implicated in many studies of schizophrenia
(7). One of the main outputs of the anterior nucleus is to the cingulate gyrus, which is also considered a portion of the limbic system and has been reported to show low rGMR in schizophrenia
(54).
The mediodorsal nucleus of the thalamus constitutes the most prominent subcortical afferent to the prefrontal cortex
(55), with which it is intimately associated
(13,
56,
57). Indeed, some researchers have defined prefrontal cortex as that region receiving projections from the mediodorsal nucleus
(58,
59). Findings of both metabolic and volumetric thalamic reductions in schizophrenia that have been reported in the literature may reflect a lack of normal frontothalamic afferent activity, which might result primarily from diminished frontal activity
(60) or more generally from disturbed connections between frontal-striatal-thalamic regions. This possibility is suggested by diminished coherence of white matter tracts in the internal capsule
(61), reduced frontothalamic rGMR correlations
(62), and rGMR hypofrontality during a sensorimotor gating paradigm thought to be mediated by frontal-striatal-thalamic circuitry
(63).
The possibility that group differences in rGMR are due entirely to total thalamic volume loss and partial volume effects is unlikely because the groups did not differ in either absolute or relative total thalamic volume. The present volumetric data are consistent with those of Portas et al.
(52), who concluded that “significant differences…will emerge when only specific nuclei are considered” (p. 654). Similarly, postmortem data revealed changes in the medial dorsal nucleus rather than in the entire thalamus
(8,
9). Area measurements in MRI, typically done on a slice cutting through the dorsoventral midpoint, might be more sensitive to nuclear change at this level than total volumetric measures. The shape analysis that was done on one axial slice through the middle of the thalamus suggests the possibility that schizophrenic patients have a size reduction in the left anterior nucleus region, whereas patients with schizotypal personality disorder have a reduction in the right mediodorsal nucleus region. While changes in total volume were not significant, it is still possible that thalamic volume reduction or reduction in another nucleus contributes to the outline position and to the anterior change.
The possibility that changes in thalamic size could be entirely drug related is raised by a report
(64) of caudate enlargement after neuroleptic treatment. However, we previously observed MRI-assessed decreases in the right anterior region in never-medicated patients
(1). Pakkenberg
(8,
9) did not find medication history related to percent volume loss in postmortem studies. Last, postmortem biochemical studies
(65) found elevated dopamine levels in the thalamus of schizophrenic patients, but not in neuroleptic-treated patients with Huntington’s disease.
Poor task performance could be related to the significantly lower thalamic rGMR in schizophrenic patients than in patients with schizotypal personality disorder and normal subjects. Overall, the schizophrenic group performed at above chance levels, however, and had higher serial-order scores than the normal group. The patients’ use of the serial-ordering strategy indicates that they were actively engaged in the task (although the semantic-clustering strategy would have been a more efficient approach). In our previous report
(1), which also found lower thalamic metabolism in schizophrenic than in normal groups, there were no statistically significant between-group differences in scores on a visual continuous performance test. Moreover, lower thalamic metabolism in schizophrenia has also been found in PET studies carried out under resting conditions
(25–
27).
Among the patients with schizophrenia and schizotypal personality disorder, reduced thalamic rGMR, particularly in the left mediodorsal and pulvinar regions of the thalamus, was associated with higher BPRS scores on the day of the PET scan. This finding suggests that disruptions in these selective subregions of the thalamus and their interconnected neural circuits play an important role in the production of symptoms in the schizophrenia spectrum.