The current study is designed to address the need for more research on attention bias in children that directly extends previous research in adults. Adult anxiety disorders have been conceptualized as conditions that emerge gradually during development
(9,
10), based on data linking adult anxiety to high levels of childhood anxiety symptoms and to adversity during childhood. Given that threat bias is thought to emerge early in the course of anxiety disorders, it is vital to extend to children available research paradigms currently used to study adults. Findings of a few preliminary studies
(11–
13) suggest that biases in attention occur in pediatric anxiety disorders, including PTSD. However, few studies examined children with clinically significant PTSD or children exposed to extreme stress in general or high levels of maltreatment in particular. Recent findings in adults
(14,
15) suggest that extreme childhood domestic physical or sexual abuse shows particularly strong associations with measures of abnormal brain function and PTSD. However, these findings derive from retrospective reports in adults; data are needed regarding the associations among extreme stress, PTSD, and threat bias in children.
Studies in adults have implemented picture-based visual-probe tasks to quantify effects of threatening stimuli on attention
(2,
18,
19). Such paradigms manipulate threat by using angry faces, a potentially more ecologically valid stimulus set already employed in developmental psychopathology research
(16). Specifically, considerable previous research documents abnormal responses to angry facial displays in maltreated children
(20–
22). This includes a reduced threshold for anger detection, disruption in attention from angry faces, and greater cognitive interference from angry faces. Nevertheless, these studies generally have not used face-processing tasks to examine maltreated children with PTSD, nor have they employed tasks previously used in adults.
The use of picture-based visual probe tasks may facilitate efforts to integrate research on adult anxiety, pediatric anxiety, and cognitive neuroscience, given that many recent neuroscience studies used evocative facial displays to study emotion
(6,
23–25). These studies found that angry faces are capable of capturing attention, evoking emotion, and engaging brain regions involved in interactions between cognitive and emotional processes
(24). In research with children, the most consistent previous findings document associations between abnormalities in the processing of angry faces and maltreatment, independent of psychiatric diagnosis
(22). Therefore, the current study tests the hypothesis that increasingly high levels of childhood maltreatment specifically are associated with increasingly abnormal threat-related attention bias. Moreover, since studies in adults relate attention bias to PTSD, the current study also tests the hypothesis that PTSD in children is associated with threat bias. We tested these hypotheses using a visual-probe paradigm previously used in adults
(26,
27). This facilitates efforts to integrate research in children and adults on the relationship between maltreatment and attention orientation.
Method
Subjects
Subjects were drawn from a larger study on trauma (Permanency Planning: Service Use and Child Outcomes; Joan Kaufman, Ph.D., principal investigator). The group of participants comprised 34 children 7–13 years old who had been maltreated and 21 children in the same age range who had not been maltreated. All maltreated children had been exposed to severe domestic abuse, defined according to standardized procedures described later in this article. All of the maltreated children had been removed from their homes for ethical and legal reasons because of the extreme nature of the abuse. The decision to remove the child was made by the State of Connecticut Department of Children and Family Services. In all cases, the state had court-awarded custody.
Comparison subjects met three criteria: no history of a maltreatment report in the Department of Children and Families; no evidence of maltreatment based on a standard assessment of maltreatment, described later in this article; and household income of $30,000 or less.
Procedures
Both the Yale University Human Investigations Committee and the State of Connecticut Department of Children and Families Institutional Review Board approved this study. Department of Children and Families caseworkers described the study to birth mothers of maltreated children and obtained permission for the research staff to contact the birth mother. Ninety-five percent of the women who were approached by the caseworkers agreed to participate. Community comparison subjects were recruited through advertisements. Clinical measures were collected within 2 weeks of the neuropsychological measures.
Psychopathology
Self-reports of anxiety symptoms were obtained by using the Screen for Child Anxiety Related Emotional Disorders
(28), which consists of written statements about anxiety symptoms that children indicate either applied or did not apply to them. Teacher reports of psychopathology were acquired by using the Child Behavior Checklist Teacher Report Form
(29), a standardized measure including 112 statements that a teacher rates as either applying or not applying to the student. A structured psychiatric interview (the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version [K-SADS-PL] [30]) was administered to each child and a parental informant.
Final diagnoses were derived by using the best-estimate procedure
(31), which involved a review of all clinical material during a multidisciplinary team meeting chaired by an expert in childhood maltreatment and assessment of childhood psychopathology (J.K.). Clinical material included results from self-reports, teacher reports, and the structured interview. Final diagnoses were assigned by consensus agreement at this meeting. For PTSD, children were diagnosed as either definitely (N=22) or probably (N=7) affected. The probable diagnosis was based on the presence of impairment and at least 85% of the required symptoms.
Maltreatment
Information on maltreatment was collected from multiple sources. Complete Department of Children and Families case records were reviewed. Birth parents completed a standardized questionnaire assessing level of domestic violence
(32). The PTSD section of the K-SADS-PL, administered to both children and parents, surveyed a range of traumas. Children’s self-reports also were obtained
(33), and additional incidents of maltreatment were reported during contact with children and families.
To reduce the number of statistical tests, the data from these five sources were synthesized by using established procedures to derive two 4-point (0=no maltreatment; 3=extreme maltreatment) scales
(32,
34). Based on results from previous studies on face perception
(20,
21), one scale rated severity of physical abuse and the other rated severity of physical neglect (interrater reliability [intraclass condition (ICC)] for physical abuse was 0.87; ICC for neglect was 0.84).
Attention Bias
A visual-probe paradigm was used that had been employed previously in research among adults
(27). Stimuli were identical to those used to study adults. Stimuli were presented by using the E-Prime software program (Psychology Software Tools, Pittsburgh) on a laptop computer in a darkened room. Subjects sat 50 cm from the computer. Testers were blind to all clinical data. The task relied on photographs of face-pairs from 64 different actors (half of whom were men), each presenting two facial expressions, one neutral and the other either angry/threatening or happy. The photographs were selected because they displayed particularly characteristic threatening or happy poses
(27).
The task began with 32 practice trials followed by 80 trials presented in random order; reaction time data were collected during these trials. For the critical 64 trials, pairs of pictures from the same actor were presented to the right or left of the screen, one picture displaying an emotional expression and the other displaying a neutral expression. These 64 trials included 32 threatening trials and 32 happy trials; one-half of the trials displayed the emotional expression on the right, and the other displayed the emotional expression on the left. An additional 16 trials displayed pairs of neutral faces. Each trial began with a 500-msec centrally presented fixation cross and was followed by a face-pair presented for 500 msec. Immediately after, a single-asterisk “dot-probe” was presented for 1100 msec on the left or right side of the screen. Subjects were instructed to press one of two keys as quickly and as accurately as possible to indicate the location of the probe (right versus left). The intertrial interval varied randomly between 750 and 1250 msec.
Data Analysis
As previously described
(19,
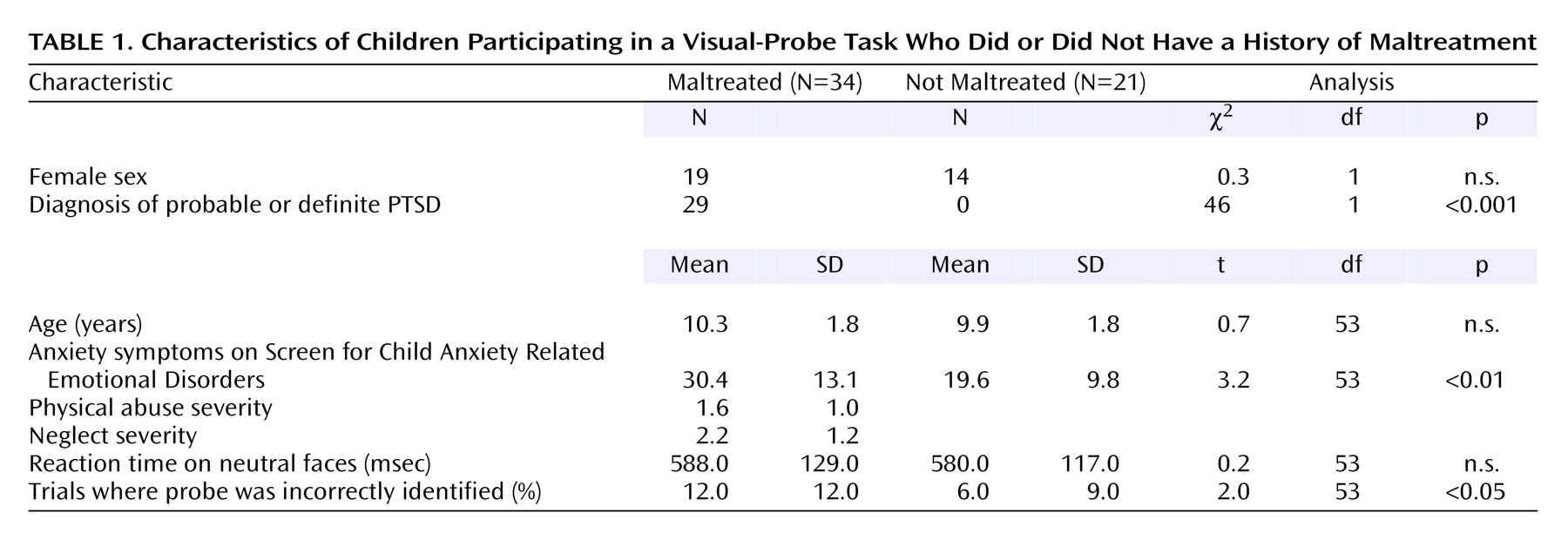
27), trials with errors were discarded, as were trials with latencies <200 msec or more than two standard deviations above each participant’s mean latency. Error rates are presented in
Table 1. Less than 10% of trials involved latencies <200 msec or more than two standard deviations above the mean latency.
We entered the study with clear a priori hypotheses based on previous data relating clinical measures to measures of attention bias to threat. As a result, analyses were based on derived measures of attention bias. These were calculated by using a standard formula
(11,
27,
35) that subtracts, for each participant, the mean reaction time on trials where the emotion face and probe appeared on the same side of the display from the mean reaction time on trials where the emotion face and probe appeared on the opposite side of the display. Positive bias scores reflect the tendency to monitor the emotional stimulus, and negative bias scores reflect the tendency to avoid the emotional stimulus.
The primary analyses examined attention bias for threatening faces. Secondary analyses examined attention bias for happy faces, reaction times on neutral face trials, and errors in probe location identification. The relationship between attention bias and maltreatment was examined in the initial set of analyses, and the relationship between attention bias and PTSD was examined in the second set of analyses. These associations were examined by using independent-sample t tests, analysis of covariance (ANCOVA), and Pearson correlations. Since we entered the study with a priori hypotheses relating attention bias to maltreatment and PTSD, statistical inference relies on two-tailed tests, alpha set at 0.05, without correction for multiple comparisons.
Results
Characteristics of the Subjects
Table 1 summarizes the characteristics of the subjects. As shown in
Table 1, physically and emotionally maltreated children exhibited higher anxiety symptoms, higher rates of PTSD, and more errors in probe location identification. No differences emerged in their reaction times to neutral-neutral probe trials. Two subjects were taking psychotropic medications. Since results appeared similar with these subjects excluded, data from these subjects were retained in statistical models.
Among the 29 maltreated children with probable or definite PTSD, 21 (72%) had a history of physical abuse, five (17%) sexual abuse, and 20 (69%) neglect. Many experienced severe maltreatment; all sexually abused children were subjected to either oral-genital contact or vaginal and/or anal intercourse. Approximately one-third of the maltreated children were exposed to domestic violence involving substantial injuries to their mothers; approximately one-fifth required medical care for acts of abuse producing injuries such as fractures; approximately one-third had been abandoned.
Attention Bias
The association between level of abuse and attention bias was examined by using both categorical and continuous indicators of abuse severity. For continuous measures, correlations were examined between measures of attention bias and physical abuse or maltreatment. The correlation between threat bias and severity of physical maltreatment was significant (r=–0.40, N=34, p=0.02), but the correlation between threat bias and severity of neglect was not significant (r=–0.15). The significant correlation reflects the fact that more severely physically abused children tended to direct attention away from angry/threatening faces. No associations arose between bias for happy faces and either physical abuse or maltreatment.
For categorical measures, the association between abuse severity and attention bias was examined further by comparing attention bias in children divided into a high-physical-abuse group—children with severe physical abuse (N=21)—and a low-physical-abuse group (N=34)—comprising children with no history of physical abuse (N=21) or minimal history of physical abuse (N=13). This designation was based on ratings from the 4-point physical abuse scale: ratings of 0 and 1 indicated low levels of abuse and ratings of 2 or 3 indicated high levels of abuse. This analysis found that the 21 children in the high-physical-abuse group exhibited significantly greater avoidance of threatening faces (mean=–22 msec, SD=48) than the 34 children in the low-physical-abuse group (mean=12 msec, SD=43) (t=2.7, df=53, p=0.009).
To examine associations with PTSD diagnosis, children were divided into two groups—abused children with PTSD (N=29) and children with no history of abuse and no psychiatric diagnosis (N=17). For this analysis, four children who had not been abused but who had psychopathology were excluded, as were five children who had been abused but did not have PTSD. Because children with PTSD tended to be older, differences in threat bias were examined by using ANCOVA, with age and PTSD status as predictors. This analysis found significantly greater avoidance of threat in abused children with PTSD (mean=–10 msec, SD=46) than in nonabused children with no psychiatric diagnosis (mean=16 msec, SD=43) (F=5.1, df=1, 44, p=0.03). Age also significantly predicted threat bias, with greater avoidance of threat in younger children (F=5.5, df=1, 44, p=0.02). Since 20 of the 22 severely abused children met criteria for PTSD (χ2=18, df=1, p<0.001), too few subjects were available to contrast threat bias meaningfully in children cross-classified with respect to both severe abuse status and PTSD diagnosis. Threat bias exhibited no association with anxiety symptoms determined by scores on the Screen for Child Anxiety Related Emotional Disorders.
Discussion
The main finding in this study is an association between maltreatment and attention avoidance of threatening faces in 34 children who had been abused. Attention avoidance of threat also was associated with a diagnosis of PTSD. However, since a large majority of the children who had experienced severe abuse also met criteria for PTSD, we could not determine whether associations with attention avoidance reflect primarily relationships with severity of abuse independent of PTSD or the presence of PTSD.
Previous studies of maltreated children document distortions in information processing of angry facial displays. These distortions include a hostile attributional bias, manifest as a lower threshold for detecting anger in ambiguous facial displays and hostility in social situations
(36), as well as high rates of emotion misidentification, attention bias, and greater interference in concurrent psychological processes
(20). However, these studies of children generally did not employ paradigms used previously in adults with a history of psychopathology or maltreatment. Moreover, these studies did not examine children with known diagnoses of PTSD or children exposed to levels of domestic abuse of sufficient severity to necessitate removal of the subject from the home.
The current study demonstrates associations among PTSD, trauma, and attention away from angry faces using a paradigm already used extensively in research on adult psychopathology and cognitive neuroscience. This allows a tighter integration of findings from the fields of developmental psychopathology, adult psychiatry, and cognitive neuroscience.
Interpretation of the current findings can be placed in the context of an extensive set of previous studies of anxiety using the visual-probe paradigm. A few studies have used verbal stimuli to examine attention bias for threat in different pediatric anxiety disorders, including PTSD
(11,
12,
37,
38). Although findings remain somewhat inconsistent, children with anxiety symptoms or disorders have been shown to differ from both psychiatrically healthy and depressed children. Nevertheless, effect sizes were relatively small, and the exclusive reliance on verbal stimuli complicates interpretations. A larger set of studies examined adult anxiety disorders, including a growing series of studies using angry facial displays or other evocative photographs
(2,
18,
19,
26,
27,
35). In fact, these paradigms have been used in adults to examine the relationship between attention bias for threat and anxiety, although not specifically PTSD
(19,
26,
27). In these studies, the most consistent finding is an association between high levels of trait anxiety and an attention bias
toward threat stimuli, including angry facial expressions. Nevertheless, other studies have found the opposite result in adult social phobia, manifest as bias away from threat stimuli
(39).
The current study found that high levels of maltreatment or a diagnosis of PTSD was associated with an attention bias
away from threat stimuli. Multiple explanations might account for differences between the current results and previous studies in adult anxiety disorders. For example, the current paradigms have not been used in research on adult PTSD or interpersonal violence. Some anxiety disorders, such as generalized anxiety disorder, may be associated with a bias toward angry faces, whereas others, such as PTSD or social phobia, may be associated with a bias away from angry faces
(39). Regardless, results from both the current study in maltreated children and previous studies in anxious adults consistently use angry faces to document associations between anxiety and attention bias. This emphasizes the need to conduct integrative studies using parallel methods in children and adults to clarify the nature of these associations across diagnoses and age groups.
The current study should be considered in the light of four limitations. First, for ethical reasons, it was not feasible to obtain data on attention bias in a group of children recently exposed to severe domestic abuse who had not changed residence. Current clinical and legal guidelines require health care professionals who identify such children to notify appropriate authorities. In conditions where the presence of severe abuse is confirmed by authorities, as for the children in the current study, clinical and legal guidelines require that such children be removed from their home. As a result, in the current study, as in other studies of children exposed to recent extreme domestic abuse, abuse severity is confounded by removal from the home. Therefore, associations in the current study for attention bias may reflect the combined association with severe maltreatment and removal from the home. To disentangle these possibilities, future studies might consider implementing novel research designs. For example, a study might examine attention bias in nonabused children who changed residence for reasons unrelated to any history of maltreatment.
Second, children were recruited from child protective service agencies. This method has the advantage of selecting children with verified histories of severe domestic abuse and minimizing conflicts that arise when maltreatment is detected in research participants previously unfamiliar to protective service agencies. Nevertheless, biases could influence referral patterns. Although children were matched on relevant demographic variables, other unknown biases may exist. Hence, the current findings may apply to particular populations of referred children. Third, the study examined a relatively small number of subjects. Moreover, because the large majority of maltreated children had a history of PTSD, the degree to which attention bias relates specifically to PTSD as opposed to severe maltreatment, independent of PTSD symptoms, remains unclear. Nevertheless, these findings are important to pursue, given that previous studies generally documenting associations between maltreatment and processing of angry social cues have not examined associations with PTSD
(20,
36).
Finally, the current study represents only an initial step in examining the relationship between anxiety and underlying dysfunction in brain circuits associated with the threat response. Future neuroimaging research might evaluate the role of such dysfunction in both attention bias and associated clinical symptoms.
This study lays the groundwork for subsequent research on neurodevelopmental aspects of attention bias as it relates to clinical anxiety and maltreatment
(15). Studies in adults suggest that threatening faces modulate attention through effects on underlying brain regions previously implicated in mood and anxiety disorders
(5,
23,
24). These include the anterior cingulate gyrus, amygdala, and ventral or medial aspects of the prefrontal cortex. Pharmacological studies suggest that activity in these brain regions can be altered by manipulations of chemical systems previously implicated in mood and anxiety disorders
(5). Therefore, the current paradigms might be used to generate insights on the relationships among anxiety, trauma, and underlying dysfunction in neural systems engaged by threat stimuli. Specifically, trauma has been hypothesized to alter functioning in brain structures that modulate attention engagement during threat presentation
(6,
15). The current study documents an association between attention bias and maltreatment using a paradigm previously shown to engage the relevant brain structures
(5). Future research might examine these associations within the context of an imaging study. Moreover, the current findings document associations between attention bias and PTSD in traumatized children. Future studies might examine resilient children, consider the effects of treatment, or examine the longitudinal nature of associations among attention bias, trauma, and PTSD. Such studies might clarify the degree to which attention bias relates over time to vulnerability to stress-related psychopathology.
Finally, this study also may lay the groundwork for future clinical studies. Avoidance of threatening facial displays may contribute to repetitive dysfunctional patterns in the social lives of traumatized children. Avoidance of threatening facial photographs in the current study may show parallels to aspects of behavior during real-life social interactions. If abnormalities in attention orientation are ultimately shown to contribute to the sequelae of trauma, this observation may carry novel therapeutic insights. For example, novel treatments might specifically target underlying abnormalities in attention orientation as a means of affecting social functioning.