Placebo responses in antidepressant trials have become a critical issue for the development of novel therapeutics and the treatment of patients in clinical settings. On the one hand, increasing placebo response complicates efforts to detect signals of efficacy for new agents in the drug development setting. The average difference observed in published antidepressant trials between medication and placebo decreased from an average of 6 points on the Hamilton Depression Rating Scale (HAM-D) in 1982 to 3 points in 2008 (
1). Consequently, for most currently approved antidepressants, less than half of the efficacy trials filed with the Food and Drug Administration for regulatory approval found the active drug to be superior to placebo (
2,
3). On the other hand, practicing clinicians know that many patients will not experience sustained remission of their depression with currently available treatments (
4). Because nonpharmacologic elements of medication treatment (i.e., placebo effects and supportive care) likely cause a substantial portion of the observed response (
5,
6), optimizing the therapeutic components leading to placebo response has the potential to significantly improve treatment outcomes in clinical practice.
Given the potential benefits to be realized from modulating the amplitude of placebo response in patient care and pharmacologic research, understanding the mechanisms of action of placebo response is critically important. Placebo effects are defined as the therapeutic consequences of receiving a substance or undergoing a procedure that are not caused by any inherent powers of the substance or procedure (
7). As such, they are conceptually distinct from other factors contributing to observed placebo response (i.e., the proportion of subjects assigned to placebo who manifest ≥50% decrease in baseline symptoms), such as regression to the mean, spontaneous improvement, and rater bias (
8). In many cases, placebo effects appear to be cognitively mediated by patient expectancy (
9), which refers to an individual’s belief about whether and how much he or she will improve as the consequence of a treatment intervention. The most common procedures for experimentally manipulating expectancies and measuring their causal effects include comparing placebo to no-treatment control conditions or else administering a drug in an open versus hidden manner (
10). However, ethical considerations prevent the use of these procedures in patients with major depressive disorder.
As an alternative approach, we have argued that placebo effects can be studied meaningfully without resorting to unethical forms of deception by comparing medication response between placebo-controlled trials (i.e., one or more medications compared with placebo) and active comparator trials (i.e., one or more medications with no placebo group) (
11). In adults and older adults with major depressive disorder, mean medication response rates in comparator trials are significantly greater than the mean medication response rates in placebo-controlled trials (
12,
13). Patients in comparator trials know they have a 100% chance of receiving an active medication, which may increase their expectancy of improvement, leading to enhanced placebo effects and greater observed antidepressant response. Consistent with these results, Papakostas and Fava (
14) reported that the probability of receiving placebo in a clinical trial correlated inversely with antidepressant and placebo response, and Sinyor et al. (
15) found that medication response was significantly higher in drug-drug (i.e., comparator) studies (65.4%) compared with drug-drug-placebo studies (57.7%) and drug-placebo studies (51.7%). These retrospective analyses suggest, though do not provide causal evidence, that the design of a clinical trial shapes patients’ expectancies of improvement during the trial, which in turn influence response to antidepressant medication and placebo.
In a prior pilot study, we found that depressed patients receiving citalopram under comparator conditions had significantly greater expectancy and improved clinical outcome compared with patients receiving placebo-controlled citalopram (
16). The present study follows up these findings in a larger trial designed to provide causal evidence for patient expectancy as a source of placebo effects in antidepressant clinical trials. Outpatients with major depressive disorder were randomly assigned to open administration (i.e., 100% probability) of citalopram compared with placebo-controlled administration (i.e., 50% probability) of citalopram, and expectancy and depressive symptom scores were followed over 8 weeks of acute treatment. We hypothesized that participants randomly assigned to open citalopram would have greater expectancy of improvement and experience greater reductions in depressive symptoms compared with those randomly assigned to placebo-controlled citalopram. Furthermore, we hypothesized that patient expectancy would mediate the depression outcome difference between these medication-treated groups at study endpoint, such that increases in expectancy would produce greater reductions in depression symptoms. Based upon the rationale that older age may be associated with structural and functional brain changes influencing patient expectancy, we planned to explore whether age moderated the magnitude of expectancy effects observed.
Method
Participants
This study was conducted at the Adult and Late Life Depression Research Clinic at the New York State Psychiatric Institute (NYSPI) and approved by the NYSPI Institutional Review Board. All participants met eligibility criteria and signed informed consent to participate in the study. Below we report clinical findings from the study, but functional MRI data were also collected and will be presented in subsequent papers.
Eligible participants were men and women aged 24–65 years old who met DSM-IV (
17) criteria for nonpsychotic major depressive disorder, had a 24-item HAM-D score ≥16, were right-handed, had no contraindications to MRI, were using appropriate contraception if they were women of child-bearing age, and were willing to and capable of providing informed consent and complying with study procedures. Individuals were excluded from participation if they were diagnosed with a current comorbid axis I DSM-IV disorder (other than nicotine dependence, adjustment disorder, or anxiety disorders), substance abuse or dependence within the past 12 months, or a lifetime history of psychosis or mania. Other exclusion criteria included the presence of significant suicidality (HAM-D suicide item score >2), a history of allergic or adverse reaction to citalopram, nonresponse to adequate trial of citalopram within the current depressive episode, current treatment with psychotherapy, Clinical Global Impressions Scale (CGI) score of 7 at baseline, current or recent (within the past 4 weeks) treatment with any psychoactive medications, or acute, severe, or unstable medical illness.
Study Design
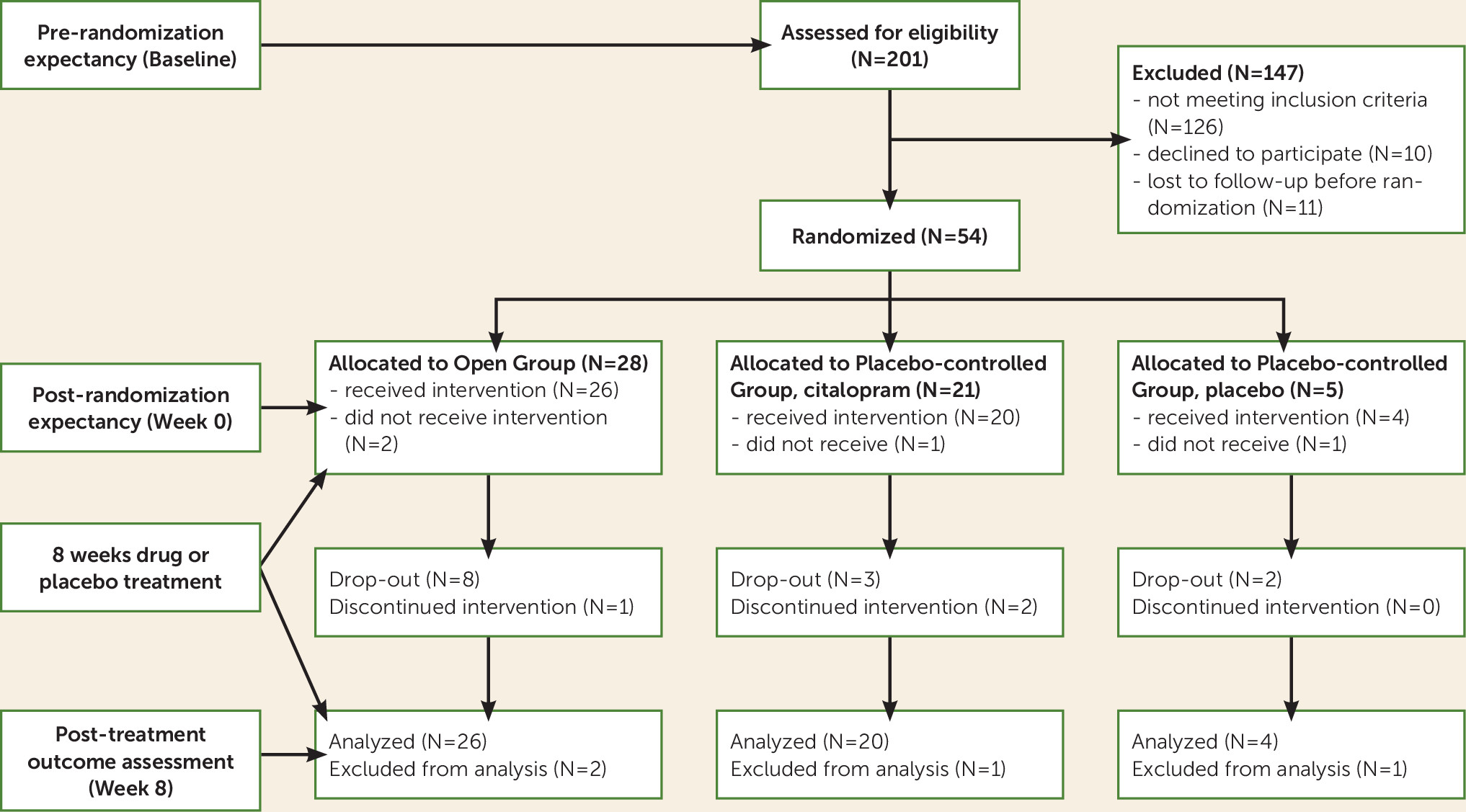
Participants were enrolled in an 8-week duration antidepressant clinical trial in which they were randomly assigned to a placebo-controlled group or open group (see
Figure 1). Participants were initially evaluated at a baseline visit, in which eligibility was assessed and prerandomization expectancy and depression scores were measured. Approximately 1 week later, they returned for a week 0 visit, during which they were randomly assigned, postrandomization expectancy and depression scores were measured, and either medication or placebo was distributed. Thus, both pre- and postrandomization expectancy were measured prior to participants receiving any study medication. They then began the study medication and returned for eight weekly visits.
Expectancy Manipulation
Expectancy was manipulated via instructions to participants about the probability of receiving active medication compared with placebo. As shown in
Figure 1, participants at baseline had what they perceived to be a 75% probability of receiving active antidepressant medication. Prerandomization expectancy was measured with subjects having this knowledge. Then, they were randomly assigned either to the placebo-controlled group (50% chance of receiving active treatment) or to the open group (100% chance of receiving active treatment) and informed of the results of this randomization. Postrandomization expectancy was measured with participants having this additional information. Those within the placebo-controlled group were randomly assigned to medication or placebo with a 4:1 ratio favoring medication, which maximized the sample sizes for the primary comparison of interest (i.e., placebo-controlled citalopram compared with open citalopram). This second randomization within the placebo-controlled group was blinded, and neither participants nor outcome assessors were aware of the 4:1 randomization schedule or the specific treatment assignment to medication or placebo.
While participants were informed of their group assignment (since this was the study’s means of manipulating expectancy), outcome assessors were blinded to group. To conceal group assignment from raters in this study, we developed a scripted method of instructing participants not to divulge this information and study raters not to request it. We also conducted checks throughout each subject’s participation in the study to determine whether the blind was broken. Those in the placebo-controlled group were informed as follows: “You have been randomly assigned to the placebo-controlled group of the study. This means that there is a chance you will receive the antidepressant medication citalopram for the duration of the study. Citalopram has been proven effective for the treatment of depression in patients like you. There is also a chance you will receive placebo for the duration of the study. A placebo is a sugar pill that is not specifically effective for depression. Neither you, nor your doctors, will know whether you are receiving citalopram or placebo. If it can be avoided, please do not reveal to anyone in the study the group to which you have been assigned.” Participants in the open group were informed as follows: “You have been randomly assigned to the open group of the study. This means that there is a 100% chance you will receive the antidepressant medication citalopram for the duration of the study. Citalopram has been proven effective for the treatment of depression in patients like you. You will not be receiving any placebo pills for the duration of the study. While you are aware that you are receiving actual antidepressant medication and not placebo, other study personnel do not know whether you are taking citalopram or placebo. If it can be avoided, please do not reveal to anyone in the study the group to which you have been assigned.”
Antidepressant Medication
Following the randomization procedures described above, participants were prescribed citalopram (20 mg/day) or pill placebo. We selected citalopram for use in this study based on its established efficacy in major depressive disorder, a favorable side effect profile, minimal drug-drug interactions, and cost effectiveness (
18,
19). If participants did not meet remission criteria (HAM-D score ≤7) after 4 weeks, the citalopram dose was increased to 40 mg for the remaining 4 weeks of the study. Subjects were aware of the potential for dosage increase at week 4 and that individuals randomly assigned to placebo would simply continue to receive placebo. Those unable to tolerate the increased dose of medication had their dosage reduced to the maximum previously tolerated dose. Absence of remission was selected to trigger dosage increases, since remission is a clinically meaningful outcome denoting the absence of significant depressive symptoms and reduced risks of recurrent depression and adverse medical outcomes (
20,
21). In the case of severe insomnia, participants were permitted to receive zolpidem (10 mg/day).
Study Assessments
At baseline, patients were screened for significant medical problems with a medical history and physical examination, a blood sample for screening laboratories, an electrocardiogram, and urine toxicology. Vital signs were recorded at baseline and weekly thereafter.
Structured Clinical Interview for DSM-IV Axis I Disorders (SCID) (
22) was performed at baseline to confirm subject eligibility. The 24-item HAM-D (i.e., the version containing items for diurnal variation, depersonalization, paranoid feelings, helplessness, hopelessness, and worthlessness) was performed at every study visit, and change on the HAM-D was defined a priori as the primary clinical outcome measure. Response (≥50% decrease in baseline HAM-D score) and remission (week 8 HAM-D score ≤7) were defined for secondary analyses. Other weekly assessments included the Hamilton Anxiety Rating Scale, Quick Inventory of Depressive Symptomatology 16-item self-report, the CGI-Severity and CGI-Improvement scales, a rating scale for treatment-emergent side effects, weekly pill counts, and a clinician and patient-rated blind assessment.
Expectancy was measured before randomization to group (baseline) and after randomization to group but before medication administration (week 0). The measure used to assess expectancy was a modified version of the Treatment Credibility and Expectancy Scale (
23), which is a widely used measure of expectancy and has demonstrated good psychometric properties in multiple studies (
24,
25). For our measure of expectancy, we used the subset of Credibility and Expectancy Scale items pertaining to expectancy (i.e., rather than treatment credibility), and we have previously demonstrated this modified Credibility and Expectancy Scale to be sensitive to differences in expectancy when subjects know they are receiving active medication as opposed to possibly receiving placebo (
16). These items ask respondents the following questions: “I believe the chances of my depression being completely better at the end of this study are …” and “Compared with now, I think my depression at the end of this study will be ….” Both questions are rated on Likert scales from 1 to 7 and summed to create the score. Anchors correspond to very poor (much worse), somewhat poor (worse), slightly poor (worse), no different, slightly good (better), somewhat good (better), very good (much better).
Data Analysis
To test for balance between randomized groups in demographic and clinical measures, two-sample t tests were used for continuous measures and Fisher’s exact tests for categorical variables. Associations between demographic factors and prerandomization expectancy were tested using one-way analysis of variance. Within-group tests of change in expectancy from pre- to postrandomization were obtained by regressing pre- and postrandomization expectancy as repeated measures predicted by group, time (pre- versus post-), and group-by-time interaction, as well as week 0 HAM-D values. The effect of randomized group on expectancy was tested by regressing postrandomization expectancy values on randomization group and week 0 HAM-D scores.
Chi-square tests compared response and remission rates between the two groups. Mixed-effects modeling was used to test group differences in HAM-D scores over time, including group, week, and their interaction as predictors, while also adjusting for gender, age, ethnicity, and week 0 HAM-D scores, as covariates, as well as an indicator for whether or not the subject was given placebo. Post hoc contrasts from a mixed-effects model treating week as categorical were used to test mean group differences at each follow-up week. To explore whether age moderated group differences, an age (treated as continuous) by group-by-week interaction was also added to the model. Contrasts were formed from the model for group differences at fixed ages (i.e., 25, 45, 55, 65) to facilitate interpretability of the age interaction effect.
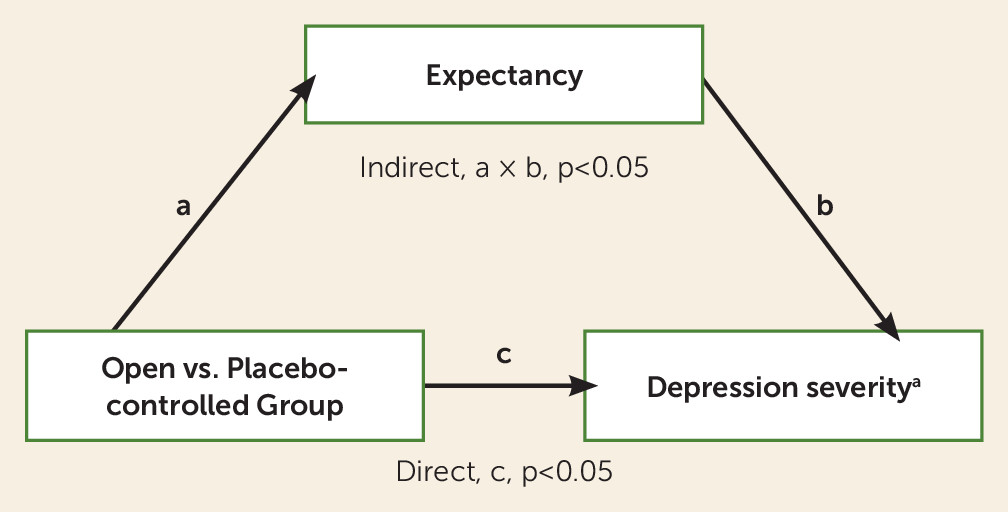
Tests for mediation of the group effect on HAM-D scores were conducted using structural equation modeling, with group as a predictor of both postrandomization expectancy (see path a in
Figure 2) and week 8 HAM-D scores (see path c in
Figure 2) and with postrandomization expectancy also predicting week 8 HAM-D score (path b in
Figure 2). Models for both postrandomization expectancy and week 8 HAM-D scores controlled for week 0 HAM-D scores, and the model for week 8 HAM-D scores additionally controlled for an indicator of whether the patient received placebo or medication to account for the therapeutic effects of citalopram. To investigate whether the mediation effect of expectancy varied as a function of self-report compared with rater-administered outcome measures, the analyses were repeated using week 8 Quick Inventory of Depressive Symptomatology 16-item self-report as the outcome. Structural equation modeling was performed using MPlus version 7.3. All other analyses were conducted using SAS 9.4 (SAS Institute, Inc., Cary, N.C.). Statistical significance was determined at a p level <0.05.
Results
Participant Disposition and Characteristics
The final CONSORT diagram for the study is shown in
Figure 1. Fifty-four subjects participated in the study, of whom four were lost to follow-up prior to taking the study medication and were excluded from the analyses. For participants in the open group, the mean age was 41.4 years (SD=12.0), 34.6% were male, the mean 24-item HAM-D score was 25.7 (SD=5.5), the mean Quick Inventory of Depressive Symptomatology self-report score was 19.7 (SD=5.2), and the mean CGI-Severity score was 4.4 (SD=0.6). For participants receiving citalopram in the placebo-controlled group, the mean age was 43.8 years (SD=10.7), 50.0% were male, the mean 24-item HAM-D score was 25.7 (SD=4.1), the mean Quick Inventory of Depressive Symptomatology self-report score was 19.8 (SD=7.2), and the mean score on the CGI-Severity was 4.3 (SD=0.5) (see
Table 1). For participants receiving placebo in the placebo-controlled group, the mean age was 34.3 years (SD=10.2), 25% were male, the mean 24-item HAM-D score was 23.8 (SD=2.8), the mean Quick Inventory of Depressive Symptomatology self-report score was 17.8 (SD=7.5), and the mean score on the CGI-Severity was 4.3 (SD=0.6). No significant differences were observed between individuals receiving citalopram in the placebo-controlled and open groups on the bases of demographic data or clinical characteristics.
Expectancy Manipulation
Mean prerandomization expectancy scores, which did not differ significantly between groups (p=0.301), were 11.2 (SD=1.1) for the open group (range: 7.0–14.0) and 10.8 (SD=1.9) for the placebo-controlled group (range: 7.0–12.0). Prerandomization expectancy did not differ between subjects on the basis of sex (F=0.511, df=1, 48, p=0.478), ethnicity (F=0.272, df=1, 48, p=0.604), or educational attainment (F=0.220, df=4, 44, p=0.926). Adjusting for week 0 HAM-D scores, the randomization to group significantly increased expectancy scores in the open group (t=3.45, df=23, p=0.002), whereas no significant change was present in expectancy scores in the placebo-controlled group (t=0.45, df=23, p=0.654). Postrandomization expectancy scores were significantly higher in the open group (mean=12.1 [SD=2.1], range: 6.0–14.0) compared with the placebo-controlled group (mean=11.0 [SD=2.0], range: 6.0–12.0; t=2.32, df=45, p=0.03), when adjusted for week 0 HAM-D scores. Thus, the experimental design succeeded in manipulating expectancies.
Clinical Outcomes
Response rates were 25% for placebo-controlled placebo, 45% for placebo-controlled citalopram, and 53.8% for open citalopram (Pearson’s χ2=1.276, df=2, p=0.528). Remission rates were 0% for placebo-controlled placebo, 20% for placebo-controlled citalopram, and 34.6% for open citalopram (Pearson’s χ2=2.783, df=2, p=0.249).
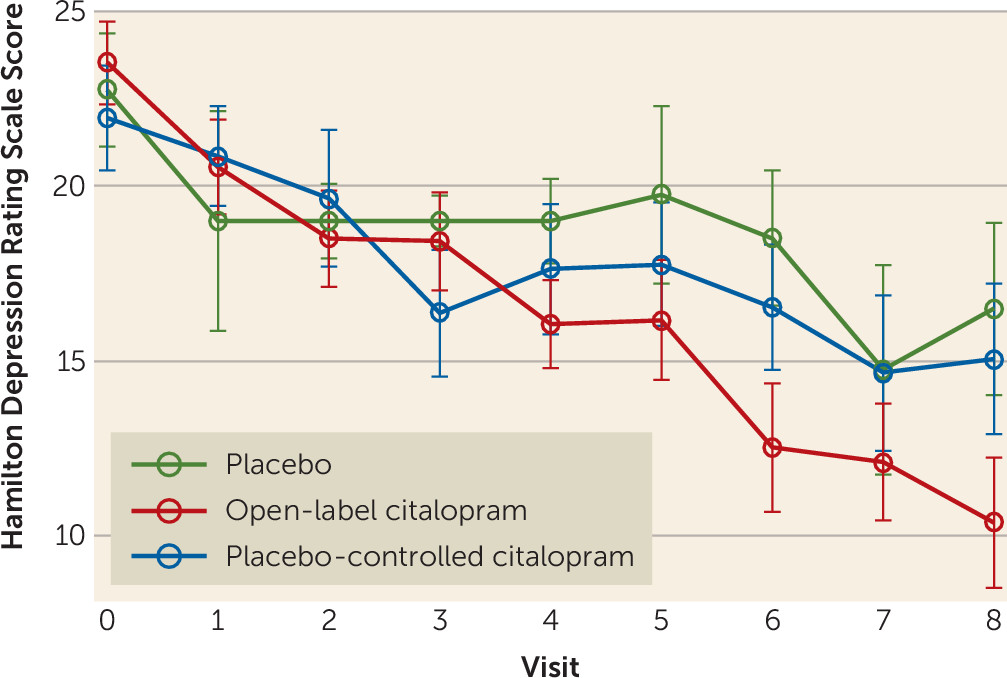
In the mixed model of HAM-D scores containing variables for group, week, week-by-group, placebo indicator, and week 0 HAM-D values, the week-by-group interaction was significant (F=8.61, df=1, 296, p=0.0036). HAM-D scores declined over time at a faster rate in the open group compared with the rate among citalopram and placebo-treated subjects in the placebo-controlled group (see
Figure 3). No benefit of citalopram compared with placebo was observed (F=0.01, df=1, 296, p=0.99), likely because very few subjects received placebo (N=4). Examination of weekly contrasts showed that participants in the open group had significantly lower HAM-D scores starting at week 4 and continuing through week 8. Adjusting for covariates, the average participant treated with citalopram in the open group experienced 6.2 points of additional improvement by week 8 compared with the average participant treated with citalopram in the placebo-controlled group. Repeating the analyses using the 17-item HAM-D resulted in a similar pattern of results.
Because we anticipated that the presence of vascular lesions and executive dysfunction (which were not directly measured in this study) may influence the magnitude of expectancy effects, we explored whether age moderated the group effect on HAM-D score by adding the three-way interaction term week-by-age-by-group to the model of HAM-D scores. This interaction was significant (F=5.24, 1, 294, p=0.0228). Testing weekly contrasts showed that the week-by-group effect decreased as age increased. At age 25, the average between-group HAM-D difference at week 8 was 11.2 (p=0.0016, favoring the open group), compared with 5.6 (p=0.0013) at age 45, 2.8 (p=0.248) at age 55, and –0.04 (p=0.992, favoring the placebo-controlled group) at age 65. To test whether additional participant characteristics were relevant to depressive outcomes, we also adjusted this model of HAM-D scores for sex, education, and ethnicity, but adding these variables did not substantively affect the results. It is noteworthy that the age moderation of the group effect on HAM-D score was not accounted for by older participants having longer duration depressive episodes, which might be associated with diminished expectancies of improvement. Age was not significantly correlated with duration of current depressive episode (Pearson’s r=0.062, p=0.677), and duration of current episode was not significantly correlated with either baseline expectancy scores (Pearson’s r=0.117, p=0.430) or prepost randomization change in expectancy (Pearson’s r=0.093, p=0.528).
Mediation of Clinical Outcomes by Expectancy
The standardized effects of group on postrandomization expectancy score (a=0.268, p=0.038) and of postrandomization score on week 8 HAM-D scores (b=−0.279, p=0.005) controlling for group were each significant (see
Figure 2). The direct (i.e., unmediated) effect of group on the week 8 HAM-D was c=−0.311 (p=0.012). Thus, the indirect effect (i.e., mediated effect) of group on week 8 HAM-D through postrandomization expectancy score was as follows: a×b=−0.075 (p=0.046). These values indicate that postrandomization expectancy is a partial mediator of the group effect on week 8 HAM-D scores.
In the mediation analyses using week 8 Quick Inventory of Depressive Symptomatology self-report as the outcome, the standardized effects of group on postrandomization expectancy score (a=0.360, p=0.001) and of postrandomization score on week 8 HAM-D (b=−0.238, p=0.036) remained significant, while the direct effect of group on week 8 Quick Inventory of Depressive Symptomatology self-report was c=0.07 (p=0.646). Thus, the indirect effect of group on Quick Inventory of Depressive Symptomatology self-report through expectancy was as follows: a×b=−0.086 (p=0.102), which, while similar to the indirect effect for HAM-D in size, did not reach statistical significance at the 0.05 level.
Discussion
The primary findings of this study were that participants randomly assigned to open citalopram had significantly greater improvement in depressive symptoms compared with those receiving placebo-controlled citalopram, and patient expectancy partially mediated these differences. Strikingly, despite receiving the identical antidepressant medication, being treated by the same study clinicians, and visiting the same treatment site, depressed subjects who knew they were receiving citalopram improved on average 6 HAM-D points more than those receiving citalopram who were aware they had a chance of receiving placebo. This difference between citalopram outcomes under high compared with low expectancy conditions is greater in magnitude than the typically observed differences between drug and placebo in antidepressant trials (
26,
27), testifying to the powerful influence of expectancy-based placebo effects on depressive symptoms.
By providing the first prospective, causal evidence for patient expectancy as a mediator of placebo effects in antidepressant clinical trials, this study confirms data from our pilot work and extends the findings of previous investigations. Leuchter et al. (
28) reported on a study in which participants were randomly assigned to supportive care alone, supportive care plus placebo, and supportive care plus antidepressant medication. While the randomization process did not affect expectancy, these investigators found that the pill-taking conditions were associated with more symptom improvement compared with supportive care alone. Greater patient expectancy was associated with greater improvement in the placebo condition but not the medication condition. Prior observational analyses from the National Institute of Mental Health Treatment of Depression Collaborative Study and a single-blind trial of reboxetine showed that higher patient expectation of improvement predicted greater likelihood of depression response (
29,
30). More broadly, these findings can be compared with neuroimaging studies in which expectations of increased pain relief have additive and dissociable effects to opiate analgesics on reported pain and pain-related brain responses (
31,
32).
The differential improvement between the open and placebo-controlled groups in this study became apparent starting at week 4, and this time course generates hypotheses for future study regarding the mechanisms by which expectancy influences depressive symptoms. One possibility is that expectancies may directly modulate depression-associated dysfunctions in the brain, perhaps akin to what is observed in neuroimaging studies of placebo analgesia (
9) or in conditions in which participants are asked to consciously regulate their emotional responses to stimuli (
33). Alternatively, expectancy may lead to more gradual depression improvement by mean of indirect mechanisms, such as increasing behavioral activation, improving medication compliance, or enhancing the therapeutic alliance between the patient and doctor (
34–
36). Given the delayed time course, data from this study appear to suggest that indirect mechanisms are likely to play a role in mediating expectancy effects on depression.
To the extent that expectancy mediates placebo responses in antidepressant studies, limiting patient expectancy may be a useful strategy to reduce placebo response in phase III trials. For example, designs in which patients have a higher probability of receiving placebo (i.e., 50%) may be preferable to designs randomly assigning patients to multiple active treatment arms and placebo. Conversely, the optimal strategy in clinical practice may be to combine active medication with a presentation that enhances patient expectancy, leading to greater medication response. Updated clinical management techniques may involve educating patients about the effectiveness of the prescribed medication and utilizing a confident and enthusiastic interpersonal style. Such presentations have been shown to enhance placebo effects for medical treatments, as in one study of irritable bowel syndrome (
37).
Intriguingly, we found evidence of diminished expectancy effects in older subjects, particularly those aged 55 and older. Late-life depression is associated with decreased response to antidepressant medications (
38) and is often accompanied by structural brain changes (i.e., white matter hyperintensities [
39–
41] and executive dysfunction [
42,
43]). Given these data, one might speculate whether a loss of expectancy-related placebo effects may underlie the diminished antidepressant response often observed in late-life depression. Patients with executive dysfunction may have difficulty updating and maintaining appropriate treatment expectancies in response to the information they are provided about the treatment being received. Even if they are able to form expectancies, vascular damage to frontostriatal tracts may limit the top-down modulation of limbic and striatal structures necessary for expectancies to produce change in depressive symptoms.
As in all studies, the results reported here should be interpreted in light of relevant limitations. Our study design did not permit us to differentiate the main effects of patient expectancy from expectancy-by-medication interactions. This limitation is unavoidable in depression studies given the ethical difficulties posed by using methodologies such as the balanced placebo study design, which allows expectancy and medication effects to be disambiguated (
44). The deception inherent to this strategy, particularly informing depressed patients that they will receive medication while actually giving them placebo, is problematic. Our study methods replicated three of the four cells of a balanced placebo design, allowing us to conclude that medication plus expectancy produced greater depressive symptom improvement than medication alone. Other limitations were posed by the relatively small sample size of the study, which did not hamper our ability to obtain significant results, and the asymmetric randomization strategy pursued in the placebo-controlled group. The few number of participants assigned to placebo prohibited us from meaningfully testing the medication effect (i.e., citalopram compared with placebo) or testing the influence of expectancy on placebo response.
In summary, this prospective, randomized study of placebo effects in antidepressant treatments is the first, to our knowledge, to experimentally demonstrate placebo effects in major depressive disorder that is not confounded by artifacts such as spontaneous remission, natural history, or regression to the mean. We found patient expectancy to be a significant mediator of these placebo effects. Developing interventions capable of modifying patient expectancy may reduce placebo response in the drug development setting and improve medication response in community treatment.